Alexander Fleming (1881-1955)
On streptococcal infections of septic wounds at base hospital.
50 THE LANCET,] MR.FLEMMING & DR PORTEOUS : STREPTOCOCCAL INFECTIONS OF WOUNDS. [JULY 12, 1819
=========================================================================================
Is the “Hæmolytic” Character of the Streptococcus of
Fundamental Importance—i.e., Can Non-hæmolytic Strepto-
cocci be Ignored for Practical Purposes in Wounds?
As has been stated above, the only streptococcus which
we have found to give rise to serious complications in a
wound is the “pyogenes” type, which belongs to the
hæmolytic group of streptococci, and we were forced to
consider the non-hæmolytic streptococci to be of only
secondary importance. In the more recent wounds, and
especially in the wounds in which gas gangrene had
developed, there is to be found very frequently streptococci
of the “fæcalis” type. These are not present with anything
like the same frequency in the latter cases. One of us
(A..F.) in conjunction with Douglas and Colebrook1 showed
that streptococci (and other organisms) had a powerful effect
in increasing the growth of anaerobic bacilli when grown
with them in symbiosis. It may be that these streptococci
of the “fæcalis” type have some importance in the wound
on account of this symbiotic action, but alone they do not
seem to be of any importance in wounds at the base.
What is the Source of the Streptococci Found in Wounds?
Examinations at a C.C.S. on recently inflicted wounds
have shown that in only about 15 per cent. of cases is
Streptococcus pyogenes present. Examinations at the base in
cases which have been in
more than a week reveal .
the presence of this organ-
ism in over 90 per cent. of
the wounds.
During the summer of
1918 we examined a
number of the gauze packs
removed from wounds on
arrival at the base. When
the patient had been kept
at the C.C.S. for more than
three or four days Strepto-
coccus pyogenes was present
in almost every case. These
cases correspond, therefore,
closely with the patients
who have been in base hos-
pitals for more than a few
days. Where, however, the
patient had been sent
straight on to the base after
excision of the wound we
found that Streptococcus
pyogenes was present only in
15 out of 75:cases. Although
in the majority of the packs
from these recent cases we
failed to find Streptococcus
pyogenes, we were able to
recover other microbes in
every case from those por-
tions of the packs which
came from the depths of
the wound, and often these microbes were present in very
large numbers. The microbes isolated in these cases were
chiefly anaerobic and aerobic bacilli and staphylococci.
It has been conclusively demonstrated that Streptococcus
pyogenes will grow much better than these other microbes in
the blood fluids2 such as would be found in a recently
excised wound, so that had the streptococcus been present as
a primary infection it should have been demonstrable on
arrival at the base. It is to be noted, therefore, that on
arrival at the C.C.S. 15 per cent, of the men were infected
with Streptococcus pyogenes; on arrival at the base (when
the cases had been sent straight on after operation) 20 per
cent, were infected, but after a stay at the base of a week
over 90 per cent, were found to have Streptococcus pyogenes
in their wounds. It would seem a warrantable deduction
from these observations that the streptococcal infection of
wounds is in most cases a hospital infection, and it is
probable that in the dressing of the wound the infection is
carried from one patient to another.
It has long been known that B. pyocyaneus is spread from
one patient to another in a ward by faulty technique in
dressing, as this infection is manifest to the naked eye by
the characteristic colour of the discharges. Other organisms
which spread around a ward in the same way are B. proteus
and diphtheroid bacilli. Now, as the Streptococcus pyogenes
will grow in the discharges very much more readily than
will these other organisms, it would be a miracle if it were
not spread in the same way. It is unfortunate that infection
by streptococcus does not produce any characteristic change
in the smell or colour of the discharges, as it does not
obtrude itself on the notice of the surgeon untill some
serious complication arises.
[NLS note: a graphic appears here – see image of page]
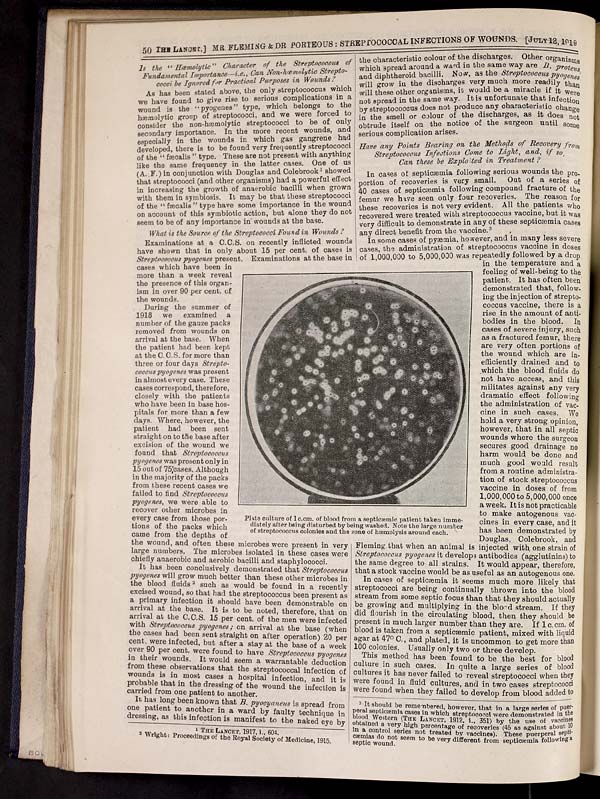
Plate culture of 1 c.cm. of blood from a septicæmic patient taken imme-
diately after being disturbed by being washed. Note the large number
of streptococcus colonies and the zone of hæmolysis around each.
Have any Points Bearing on the Methods of Recovery from
Streptococcus Infections Come to Light, and, if so,
Can these be Exploited in Treatment?
In cases of septicæmia following serious wounds the pro-
portion of recoveries is very small. Out of a series of
40 cases of septicæmia following compound fracture of the
femur we have seen only four recoveries. The reason for
these recoveries is not very evident. All the patients who
recovered were treated with streptococcus vaccine, but it was
very difficult to demonstrate in any of these septicæmia cases
any direct benefit from the vaccine.3
In some cases of pyæmia, however, and in many less severe
cases, the administration of streptococcus vaccine in doses
of 1,000,000 to 5,000,000 was repeatedly followed by a drop
in the temperature and a
feeling of well-being to the
patient. It has often been
demonstrated that, follow-
ing the injection of strepto-
coccus vaccine, there is a
rise in the amount of anti-
bodies in the blood. In |
cases of severe injury, such
as a fractured femur, there
are very often portions of
the wound which are in-
efficiently drained and to
which the blood fluids do
not have access, and this
militates against any very
dramatic effect following
the administration of vac-
cine in such cases. We
hold a very strong opinion,
however, that in all septic
wounds where the surgeon
secures good drainage no
harm would be done and
much good would result
from a routine administra-
tion of stock streptococcus
vaccine in doses of from
1,000,000 to 5,000,000 once
a week. It is not practicable
to make autogenous vac-
cines in every case, and it
has been demonstrated by
Douglas, Colebrook, and
Fleming, that when an animal is injected with one strain of
Streptococcus pyogenes it develops antibodies (agglutinins) to
the same degree to all strains. It would appear, therefore,
that a stock vaccine would be as useful as an autogenous one.
In cases of septicæmia it seems much more likely that
streptococci are being continually thrown into the blood
stream from some septic focus than that they should actually
be growing and multiplying in the blood stream. If they
did flourish in the circulating blood, then they should be
present in much larger number than they are. If 1c.cm.of
blood is taken from a septicæmic patient, mixed with liquid
agar at 47°C., and plated, it is uncommon to get more than
100 colonies. Usually only two or three develop.
This method has been found to be the best for blood
culture in such cases. In quite a large series of blood
cultures it has never failed to reveal streptococci when they
were found in fluid cultures, and in two cases streptococci
were found when they failed to develop from blood added to
_______________________________________________________
1 THE LANCET, 1917, i., 604.
2 Wright: Proceedings of the Royal Society of Medicine, 1915.
3 It should be remembered, however, that in a large series of puer-
peral septicæmia cases in which streptococci were demonstrated in the
blood Western (The Lancet, 1912, i., 351) by the use of vaccines
obtained a very high percentage of recoveries (45 as against about 10
in a control series not treated by vaccines). These puerperal septh-
cæmias do not seem to be very different from septicæmia following
septic wound.

{kind=link}
- © National Library of Scotland 2009
- NLS home page
- Digital library